
Racialized Disgender and Disruptive Futurity in Lorde’s and Engelberg’s Cancer Narratives
In an entry near the beginning of Audre Lorde’s The Cancer Journals (1980), Lorde describes her embodied experiences of diagnosis, pain, mastectomy, and hospitalization as directly connected to the intersectionality of racial and gender oppressions when she writes, “The blood of black women sloshes from coast to coast and [Mary] Daly says race is of no concern to women. So that means we are either immortal or born to die and no note taken, un-women”[2]. This moment in The Cancer Journals reinforces a central line of thinking in black feminist thought that “woman” is a racial as well as a gender category, historically constructed on the exploitation, destruction, hyper-sexualization, and ungendering of black women’s bodies resulting from historical violences such as the reproductive economy of chattel slavery and post-emancipation characterizations of black women as existing for the caretaking of or sexual exploitation by whites.[3] Hortense Spillers, in her foundational “Mama’s Baby, Papa’s Maybe: An American Grammar Book”, notes, regarding the ungendering of black women, that a primary form of dispossession resulting from slavery was “the loss of gender” and necessitates an “altered reading of gender” for black men and women in the United States (77). Spillers here outlines the specific constructions of the “ungendered” black female in the Unites States.[4] She highlights the continued social marginalizations that have occurred for black people as a result of historical exclusions from normative gender and kinship structures, as well as the radical potential of “claiming the monstrosity” of the female subjectivity that exists outside of normative American grammar.[5]
Both Spillers’ argument about historical constructions of black womanhood, as well as the quote above from Lorde, incorporate a less obvious acknowledgement of a tenant of disability studies—that the ways in which bodies are labeled and treated as disabled (particularly non-white and female-marked bodies) can strip them of access to coherent gender identity. Rosemarie Garland-Thomson expands on this connection and the ways is both limits and expands possibilities for raced and gendered subjecthood in her study of “several twentieth-century African-American women writers [who] use disabled figures in strategies of empowerment” that reclaim disability and disabled bodies from a history that has both perpetrated violence against them and used stereotypes of disability to mark them as outside a gendered norm.[6] Nirmala Erevelles has argued of Spillers specifically, that her “essay is as much about disability as it is about race” in that it is “in becoming disabled that the black body is at the height of its profitability,” and thus ungendered commodification.[7] While Garland-Thomson focuses on the reclaiming of representations of black female disability and Erevelles focuses on ways that black bodies were “transformed into a commodity—without gender, without genitalia, without subjectivity” as the “becoming disabled” of blackness, I argue in this essay that is it via the disabling process of racialized gender that culturally-informed bodies come to inhabit a disgendered and tenuous subjecthood. In other words, it is not so much, as Erevelles suggests, an “ironic twist” when “previously un-gendered” bodies are “perceived as gendered commodities” when it comes to the reproduction of the slave population. Rather, this is one particular historical and exceptionally violent and subjectivity-stripping example of the ways that disability is always at work in creating racialized disgender. I argue here that gender is not only a state one can have “stripped” from them, but a status that is always already given as a cultural and economic commodity and that both its normative and marginalizing forms are disabling in the sense that they construct racialized gendered subjects as limited both in their material selves—often as a result of physiological and psychological violence—and in their access to personal expression, political agency, and public belonging. The racialized histories of these disgendered formations inform the ways in which we read gender in the contemporary moment and contribute to reinforcing gender binaries.
As an attempt to name and assess some of the ways historically constructed racialized disgender continues to inform cultural assumptions about binary gender—assumptions that keep heteronormative, anti-queer, and white supremacist systems in place—I will explore in this essay the ways in which the intersections between modes of denying access to legible gender identity, which are oppressive in practice, might render the relationship between discourses of ability and gender normativity (which is also a raced, classed, and sexualized normativity) more legible. This, as Spiller’s suggests in her comment about “claiming the monstrosity,” could ultimately be a more liberating response than fighting for access to normative constructions of gender. Here I focus not exclusively on African American constructions of femaleness, but on multidimensional illuminations of the process of racialized disgendering that arise from the reading of two breast cancer narratives written against the grain of powerful cultural white-dominated and hegemonically feminizing discourses around the disease.
Theorizing Racialized Disgender
In the readings that follow I use Audre Lorde’s and Miriam Engelberg’s representations of gendered and raced experiences of breast cancer to explore the concept I am terming racialized disgender. I choose the prefix “dis” for “disgender” in part to highlight the relations between disability as a social construction that has functioned historically by denying access to certain bodies and then projecting that denial back onto them as a personal lack, and gender as a social construction that has functioned historically by denying access to certain bodies and projecting that denial back onto them as personal lack. I also choose the prefix “dis” as a reference to José Esteban Muñoz’s term “disidentification.” Just as Muñoz’s disidentification is neither an assimilation to dominant narratives nor a counter-identification, but a potentially subversive recircuiting of dominant narratives of identity; disgender is neither an assimilation to dominant gender identities, nor a complete rejection of or removal from dominant narratives of gender, but rather a way of thinking about the complex and disabling (in both the sense of limiting access and in the sense of providing a social identity and epistemically valuable way of being in the world) ways that gender intersects with our other social identities, here particularly race. Muñoz also describes disidentification as a “survival strategy” in that one must exist within dominant narratives of identity whether or not those narratives line up with one’s sense of themselves.[8] Disgender is also a survival strategy. We are all existing within dominant discourses of gender and become legible to others within them, whether or not we see ourselves in them or feel they are working for our safety and freedom.
Racialized disgender as a concept is not meant to coopt real material positions of disability or to make disability a metaphor for race or gender. Sami Schalk notes that it is imperative in feminist writing not to reproduce negative associations with disability by using metaphors that represent “disability as an irredeemably negative state of being.” Rather, Schalk argues, “Feminist scholars must find a way to discuss the harmful effects of patriarchy on both men and women without simplistically equating such effects to impairment.” I would like to push a little on this distinction between gender, disability, and impairment--not by erasing the differences between those categories nor that lived experiences we have within them, but rather by exploring the complexities of the ways race and gender disable and impair bodies, and the way social identities as we know them originate in the impairment and disabling of bodies along racial and gendered lines. Metaphors that associate disability or impairment with an irredeemably negative state not only alienate people with disabilities, they also undermine the perspectives and value of people with marginalized gender and racial identities.
Racialized disgendering as I use it here, then, is not so much a metaphor for race and gender as it is a description of a linguistic and ideological practice that constitutes racialized gender identity in direct relation to ideas about healthy and able bodies as well as in relation to physical, emotional, and psychological limitations on individuals—disabilities that we grow into as we learn to perform our expected gender identities. The close readings of the workings of racialized disgender in Lorde’s and Engelberg’s work attempt to parse some of the complex relationships between gender performativity, bodily policed and reinforced gender norms, ableist expectations for bodies as filtered through lenses of racialized gender normativity, and alternate possibilities for inhabiting racialized gender and gendered race, that might become more legible through experiences of bodily illness and disability. Critical readings that discuss disability, gender, and race as mutually constitutive to subjecthood, have often looked at ways that non-white bodies have been ungendered and thereby disabled, rather than thinking of racialized disgender as a broader and interconnected system that racializes and genders all bodies in ways that are so wildly disparate in their creation and denial of access to cultural, social, and economic capital, that we can only read them against and rarely in conjunction and intersection with each other. This approach, while important and necessary, does not always do as much work as it could to resist the cultural logic of a gender binary given or denied to bodies based on race, cis/trans status, class, criminal status, ability status, and citizenship, among others. Lorde’s and Engelberg’s autopathographies challenge the un-gendering binary often constructed around non-white and disabled bodies—either transcendent or futureless (in Lorde’s language: “immortal or born-to-die”)—and reveal the ways in which gender expectations themselves (and the intersecting identifications that inform them) are always already disgendering bodies. To conclude from the fact that one is denied access to dominant forms of manhood or womanhood that they are thoroughly ungendered, not only denies the realities of the ways that disabled men and women and women and men of color live their genders, but also denies the subjective experience of many intersex, non-binary, transgender, and gender queer people who do not identify as men or women.
In the readings below I will use the term “racialized disgender” to describe representations of bodies in a twofold manner. Racialized disgendering refers to: 1) Bodies that are physically, intellectually, or emotionally impaired or socially disabled by the process of racialized gendering; and 2) Bodies that are legible as being physically, intellectually, or emotionally impaired or socially disabled by the process of racialized gendering, often in combination with a status of illness or disability. One can be racially disgendered in the first sense, without being racially disgendered in the second. However, the bodies that fall into the second category help explore and highlight the racialized disgendering processes of those in the first that might otherwise remain less culturally legible. They may become sites to “explore and exploit” the relations between limiting racial and gender expectations, and ideologies of health and ability status.
Recognizing racialized disgender as it appears in narratives of illness or disability, then, is a way of both describing how gender works more broadly and queering normate gender narratives as they intersect with ableist expectations about what constitutes a healthy body. Given the well-theorized history of the creation of race and gender through disability and impairment,[9] I am interested less is showing this historical formation and more in exploring how relationships between racialized gender constructions and physical and social disability complicate our understanding both of how gender functions as a limiting discourse as well as how our attachments to aspects of an historically oppressed gender positionality such as womanhood might be revalued even as multiple classed, racialized, and sexually regulated “womanhoods” have contributed to injuring those categorized by them. I believe we need to investigate further what it means to claim the monstrosity of disgendered womanhood, a (re)claiming that I will argue questions and ultimately undermines the man/woman binary that makes womanhood a stable category in the first place but does not devalue its worth as a lived internalized and loved identity.
Thus racialized disgender as a theoretical concept moves away from binary models of gender and toward a queer framework that attempts not only to describe the construction of, but also to undo or put into question the coherence of the concept of gender, even as it recognizes binary gender’s continued social power and the frequent necessity of it for one’s full recognition as human in both institutional and interpersonal contexts. As a theoretical concept, racialized disgender works alongside concepts of gender queerness and transgender identity, while signifying something different than either and functioning in a potentially more affectively ambivalent space. It is less celebratory than gender queer or gender fluid, in that it maintains an awareness of and connection to the ways in which racialized gender, particularly but not exclusively non-white manhood and womanhood and white womanhood and girlhood, is enforced at least in part as a set of limitations and disabilities. One way this manifests is that what one cannot or is not supposed to do or what threats one’s body faces in their environment comes to define one’s social gender as much as anything else. Racialized disgender, by retaining awareness of the limiting aspect of racialized gender constructions, also acknowledges that these disabling aspects of gender can be and often are psychologically wounding to the subjects on which they are enforced. At the same time, racialized disgender is less inclined to reinforce gender binaries, ableism, and the power of the medical industry than current popular uses of transgender, which has been co-opted to a great extent by popular medical and rehabilitative models that often present transpeople as “really” male or female and simply in need of medical intervention to become their true selves—a true self that frequently and independent of the race of the transperson, is presented as “successful” in that it meets many of the normalized expectations for ideal able-bodied white manhood and womanhood.[10] The concept of racialized disgender also recognizes that ungendering has been as historically violent as hypergendering, particularly for poor women, women of color, queer women, and intersex and gender nonconforming people.[11] Racialized disgender, like disability, is a potentially universal term. We could say we are all in some way disgendered, just as we are all in some way impaired (or at least will be or have been), but just as only certain impairments register culturally as disability, only certain gender contexts and intersectionalities register culturally as disgendered. Thus the concept of racialized disgender attempts to maintain an aspect of true ambivalence around the ways oppressed gender identities have been constructed—to see them as both a source of knowledge, community, and joy, AND as a site of historical and contemporary pain, ressentiment, and limitation.
Breast Cancer as site of Racialized Disgender Narratives
Narratives of breast cancer can be productive sites to explore the concept of racialized disgender not only because they focus on a disease that is considered a woman’s illness, but also because highly gendered narratives of and around breast cancer have entered mainstream cultural discourses to the extent that breast cancer has its own month and pink ribbons have become a legible form of marketing, fundraising, and self-identifying across class, gender, race, regional, and ability statuses. While Mary K. DeShazer and Anita Helle suggest that postmillennial cancer narratives “differ from their twentieth-century counterparts” in that they address “environmental carcinogens,” “question the medical establishment,” and “challenge mainstream cancer culture,”[12] many breast cancer autopathographies replicate normative ideologies of (white) womanhood, gender conformity, and ableism in relation to a medicalized and heteronormative understanding of the normate body.
In the analyses that follow, I look at two cancer narratives that resist dominant narratives of womanhood and illness not only via the critiques mentioned by DeShazer and Helle, but by highlighting relations between mainstream ways of representing breast cancer and broader modes of racialized disgender. Engelberg and Lorde both write narratives of what Lisa Deidrich calls “politicized patienthood,” in that they recognize, criticize, and resist normative reactions to breast cancer and breast cancer patients. Lorde is consciously politicized by her involvement in feminist politics and the feminist health movements of the 1970s, and in The Cancer Journals, explores how breast cancer fits into larger systems of social oppressions through a collection of non-fiction essays and journal entries. Miriam Engelberg’s comic memoir Cancer Made me a Shallower Person (2006), is a humorous and understated critique of the ways breast cancer intersects race, gender, and what we consider normative perceptions and behaviors from the perspective of a white, straight, relatively economically privileged Jewish woman. Both texts reveal not only ways that breast cancer narratives are gendered, but also the ways that their experience of gendered illness is haunted by racial trauma. Both authors’ narratives speak to the ways in which illness can highlight our social racialization and disgendering as well as the cultural and intergenerational ways we receive our racialized disgendered selves, themselves affected by histories of political disabling, impairment, and death. Formational histories of violence and the negative affects often experienced by those who are ill, impaired, or socially marginalized are also systematically revalued by both authors, particularly in contrast to dominant medical and rehabilitative discourses and their potential to stifle access to knowledge about the ideological structuring of race, gender, and disability.
Dominant medical and rehabilitative industries work within a broader consumer capitalist system as ideological state apparatuses that enforce institutionalized surveillance that predominantly disciplines itself along the normative gendered lines. Lennard Davis terms the work of these industries care of and care for—as opposed to caring about—the body. A politics of caring about the body involves attention to the rights, treatment, and oppression of disabled, non-normative, and ill bodies, and thus would require greater attentiveness to the racially disgendering ways our bodies’ histories and social narratives disable us as well as the ways these narratives contextualize and affect the experience of disability and illness. Lorde’s and Engelberg’s autobiographical persona’s bodies are represented as racially disgendered bodies not because they are cancerous, amputated, or undergoing chemotherapy, but rather because the ways in which their bodies are marked by breast cancer reveal the ways in which various social forms of womanhood themselves are not constructed to care about women. The remainder of this essay expands on the suggestion that breast cancer is not only a gendered and gendering disease, but that a close reading of its social functioning and the rhetorics that have been used to make it less threatening to dominant understandings of both race and gender can also reveal more clearly ways that racialized gender functions as a form of disability more broadly.
Audre Lorde: Diagnosing Patterns and Responses
Lorde opens The Cancer Journals by stating that “Every woman responds to the crisis that breast cancer brings to her life out of a whole pattern, which is the design of who she is and how her life has been lived."[13] This means not only that each person brings to illness their own experiences, but that the ways in which women have learned to be women, the patterns and designs of their gender identities, are intimately related to the ways women experience breast cancer. Female illness in general is itself experienced through the same affective and responsive lenses that gender women more broadly. Particularly in the case of breast cancer, expectations associated with recovery and rehabilitation reflect expectations for ideal womanhood in dominant cultural constructions such as self-sacrifice (sometimes in the form of painful and disruptive treatments to save one’s breasts, sometimes in the physical removal of one’s breasts), making oneself an unobtrusive presence to others (the prosthetic and social/emotional covering of that loss), and making space for and attending to others’ needs before one’s own (to appear as a physiologically “normal” woman becomes more important than dealing with one’s own emotional and physical needs). Lisa Diedrich makes the point via Carole Colbourn that breast cancer is associated with the loss of body parts that matter in a patriarchal culture because they are “objects to be desired by heterosexual men and as symbols of motherhood."[14]
These are not the only dominant discourses of female worth that Lorde is negotiating. Dominant expectations for black womanhood involve self-reliance, hyper- or de-sexualization, and social caretaking beyond the immediate family. These expectations, which might otherwise register strength, power, visibility, and influence, have historically been used instead to reinforce black women’s social invisibility and lack of power.[15] The figure of the black woman has in fact historically functioned as a kind of supercrip, whether physically disabled or not—constructed through what Therí Pickens refers to as “the discourse of the superhuman survival."[16] From historical mythologies about black women’s bodies being able to handle what white women’s could not, thereby marking them as other than true women, to more contemporary stereotypes about strong black womanhood,[17] the body of the black woman has often been figured as both disabled in relation to true womanhood and simultaneously superhuman in its ability to overcome hardship.
Lorde identifies a significant portion of the “patterns and designs” of her own experience of black female identity as having been learned through the internalization of fear and vulnerability—affects associated both with dominant figurations of the sick female body and with Lorde’s marginalized queer, black womanhood. Here her experience as a queer black woman echoes and reinforces the way she is read and treated as a sick body. In response to her diagnosis of breast cancer, Lorde fears most “that [she] was not really in control” of her body and “that it might already be too late to halt the spread of cancer,” thus highlighting the ways in which illness contributes to feelings of fear and vulnerability.[18] Yet she also tells us that “[a]s women we were raised to fear."[19] And she is constantly aware of the ways her body is constructed as a particularly vulnerable object in her society by being marked black, female, and queer. Thus the experience of cancer augments the affective experiences of fear and vulnerability, but it also draws attention to the ways these emotions are socially constructed and projected onto certain bodies to be processed and experienced by the culture more broadly. Lorde suggests that if she can become aware of how as a black woman she is taught to fear, she might then become more able to be attentive to and aware of the ways that as medically diagnosed bodies, sick women are also taught to fear. And in that recognition she might potentially find a place to be less fearful, despite the real bodily vulnerabilities that exist for women of color and people with chronic or terminal illness.
When Lorde is taken into surgery she describes her body as a vulnerable object in a white-dominated medical complex. “[T]he clanging of disemboweled noises that have no context nor relationship to me…I have ceased being a person who is myself and become a thing upon a Gurney cart to be delivered up to Moloch, a dark living sacrifice in a white place."[20] This scene highlights the ways her body becomes vulnerable in terms of the power dynamics between healthy and ill bodies, white and black bodies, and male and female bodies. She will lose her black breast (a physical marker of her race and gender) to the white place, as a sacrifice to its success (in curing her) and its continued functioning (bringing in more patients to do the same to). Lorde asks us to attend to all of what must be sacrificed of oneself as a black woman in order for her to gain access to medical care. Not only is she losing her breast, but the white place itself coopts even the space of injury—it is the place that produces “disemboweled noises”—while her body, which should be the subject at the center of care, becomes a passive “thing” offered up to the injured white space. She is disallowed claim to her own illness, as it is instead claimed by the medical institution, herself becoming a sort of prosthetic used in the process of keeping the body of the white place intact
She is also metaphorically positioned as a child, in that the sacrifices offered to Moloch were often children. Barbara Ehrenreich has argued that infantilization is a part of breast cancer rhetorics more broadly, and specifically in breast cancer awareness products such as teddy bears and the relentless “it’s-a-girl” pink theming. “You are encouraged to regress to a little-girl state, to suspend critical judgement, and to accept whatever measures the doctors, as parent surrogates, choose to impose."[21] This regression is specifically encouraged for patients with “women’s illnesses,” such as breast cancer. Ehrenreich implicitly notes the function of racialized disgendering here when she suggests that perhaps, “in some versions of the prevailing gender ideology, femininity [i.e. idealized white femininity] is by its nature incompatible with full adulthood.[22] The way in which the medical industry produces vulnerability, then, is a form of created dependency that is both new for recently diagnosed patients and also an extension of the kind of social diagnoses that women, as women, have been living with their entire lives.
It is in this heightened and gendered state of vulnerability, Lorde suggests, that “many patterns and networks are started for women after breast surgery that encourage us to deny the reality of our bodies which have just been driven home to us so graphically."[23] It is Lorde’s illness that reconnects her to a sense of the reality of her body—a reality that normative gendering itself has had the effect of undoing and which is undone again after breast surgery. While all gendering involves social pressures and expectations that can disconnect a person from a sense of the needs and reality of their body, women—who have historically been represented as objects of the male gaze; caretakers for men and children; and ideally small, silent, and confined—are often particularly distanced from an embodied exploration of themselves that would attend to and privilege a physical and psychological connection to themselves. One value of the experience of illness, as Lorde represents it, is an awakening to bodily awareness that distances one from their own gendered positioning—that is, it legibly disgenders one enough to become aware of the gendered teachings that have separated one from a sense of bodily autonomy, agency, and general comfortable embodiment.
In The Cancer Journals, as Lorde becomes more aware of this pattern of disgendering, the medical and rehabilitative industries augment their ideological pressures to reinforce normative gender (i.e. compliant, white-centric, and heteronormative) performativity from her. For Lorde they find their ultimate objective correlative in the prosthetic breast, which, Lorde believes, “encourages [women] not to deal with [themselves] as physically and emotionally real, even though altered and traumatized."[24] In my reading of Lorde’s protest of the prosthetic breast, the false breast functions as both a tie to and a repression of a wounded past. The prosthetic breast ties the female patient not to the actual physical wounds of cancer or surgery, nor to the awareness of being socially and politically oppressed, but rather to the ideological wound that reproduces womanhood as a state of vulnerability and fear, and black womanhood as never fully meeting the standards for successfully embodying that feminine vulnerability. The prosthesis, Lorde says, “encourages women to dwell in the past rather than a future…and to focus [their] energies upon the mastectomy as a cosmetic occurrence, to the exclusion of other factors in a constellation that could include her own death."[25] The prosthesis functions as a reinterpellating of women, including the historical ungendering of black women through a white supremacist ideal (represented by the “grotesquely pale” lambswool Lorde is given to pad her bra), to repress traumatic histories rather than attempt to engage and process them. It encourages women to dwell in a surface history of their oppression, shame and lack of power, rather than to engage the deep history of physical violence and trauma that constituted this oppressed position and to incorporate that into their current understanding of themselves. For Lorde, the prosthesis represents a sick (disemboweled) medical environment that prefers quick fixes that reinforce the hegemonic control of institutionalized medicine and encourage individual protective (rather that group political) responses to fear and vulnerability. Lorde’s point is not about the individual women who choose to wear prosthetics or get reconstructive surgery, but about the ways these are assumed to be the only viable options. The individualized medical approach limits access to others’ experiences as well as time to consider options, and privileges professional knowledge. Covering the wound that marks the lost breast is a form of covering access to the knowledges that the histories of our wounds and the visible markers of what we have lost can provide. The values of looking at wounds include the creation of group experience and knowledge and the a prioritization of “psychic time and space to examine what our true feelings are, to make them our own," thereby incorporating the knowledge of loss and traumatic experience rather than avoiding it.[26]
Lorde’s use of phrase the “fantasy of reconstruction” to refer to immediate surgery to “replace” one’s lost breast(s) alludes historically to the national failure of post-Civil War reconstruction—a time period in which, as Jim Downs has argued, African Americans were exposed to more illnesses and physically threatening circumstances than ever before in the nation’s history and during which a newly defined population of “dependents” was created against the category of black workers.[27] The Freedman’s Bureau utilized the category of “able-bodied” to recruit men for agricultural labor and to reject from the labor population “single freedwomen, elderly, disabled, and orphaned former slaves."[28] This historical allusion grounds Lorde’s argument about her contemporary experience as a black body under the care of a white-dominated medical industry in a history of medical models designed to reconstruct and rehabilitate that have actively and aggressively prevented cohesive community for women, African Americans, and people with disabilities; undermined social changes and access to the resources that might benefit and allow healthy lives for those groups, in favor of hegemonic ideas about communal or national health; and devalued the worth and autonomy of those bodies marked female, dependent and non-able-bodied.
Contemporary ideologies of medical reconstruction and rehabilitation do similar work as by putting those who might gain access to such knowledge under surveillance with the aim to prevent their attempts at shared knowledge creation is reflected in the practices of the hospital and associated medical sites. Lorde demonstrates how a woman who does not wear a prosthetic breast is seen as a threat to the “morale” of a breast surgeon’s office and asked to hide the very wound she is there to treat.[29] Here the amputated, disabled body, is the female body itself in that the normate female body is expected to reveal itself by visibly registering certain fetishized body parts such as breasts and buttocks even as they are ostensibly hidden. The line between a tight shirt or push up bra, and the prosthetic breast Lorde is pressured to wear is a difference of degree rather than kind. Gendered and able-bodied norms work together to hide women’s bodies both before and after they are diagnosed as ill via idealized images of the female body. This hiding actually, then, reinforces a normatively disabled female body (one that already needs certain prostheses to register as properly female) and simultaneously hides that disabled status. The prosthetic breast functions in the same way, here doing potentially even more harm by hiding one’s history of immediate suffering and experiences with both illness and the infantilizing structures of the medical industry from others in one’s position, limiting possibilities for a more powerful feminist disability community and thereby more powerful feminist disability activism. Lorde survives these pressures by inhabiting and articulating her awareness of an already racially disgendered space. She not only “chooses to wear her cancer,” as Diane Price Herndell suggests, but wears her black, queer, sick, and disgendered female identity legibly when the world is asking her to hide it because of its threat to the normative racialized structures of gender that would otherwise work to render black women powerless.
Miriam Engelberg: Inherited Patterns, Disgendered Responses
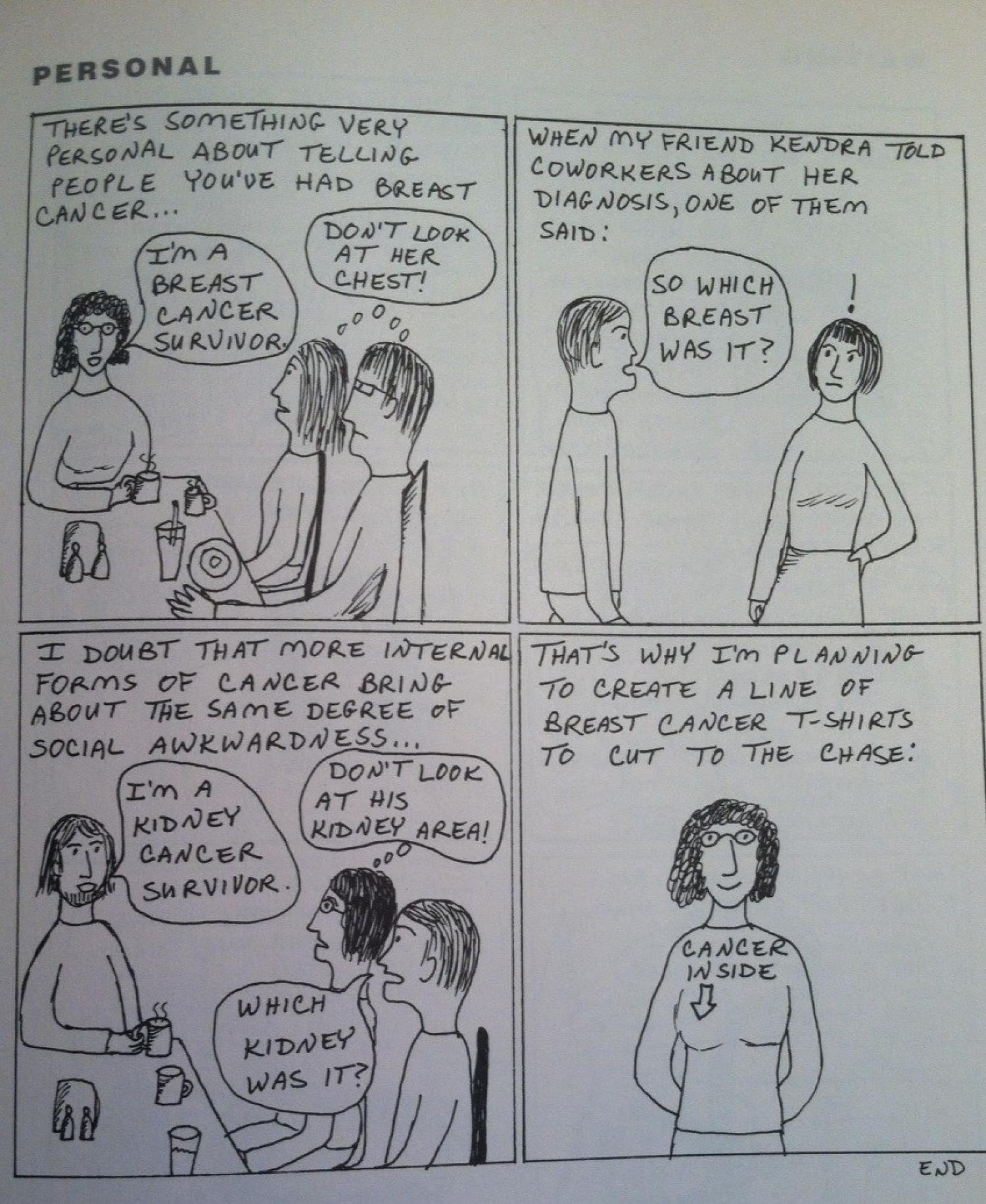
Miriam Engelberg similarly critiques the discourses and expectations of the healthcare industry and engages a history of inherited trauma and identity formation, experienced through her cancer as a form of racially gendered embodiment. Engelberg begins her comic memoir, Cancer Made Me a Shallower Person, with a set of four panels entitled “Personal,” in which she, like Lorde, plays with the idea of choosing to wear her cancer. She jokes that breast cancer, unlike more “internal forms of cancer,” brings with it the social awkwardness of people trying not to look at the woman with cancer’s chest or think about her breasts.
What is represented as “personal” in this strip is not just information that is private or revealed only to certain people, but also personal in that it refers to Miriam’s person and the way that person is already vulnerable and sexualized because of her female identity and the politics of visuality surrounding female bodies. When Engelberg jokes that more “internal” forms of cancer wouldn’t provoke the same response as breast cancer, she associates women’s illness with a surface performativity of bodily health and gender normativity. The reason that a breast is considered less internal than a liver or a lung is because of the way women’s secondary sex characteristics are read as both belonging to the woman (part of her insides) but also available for consumption, particularly by men (something she wears, projects, or gives to others). Breast cancer focuses attention on these internal/external sexualized body parts and specifically on the primary sexualized body parts that our culture asks women to partially cover but also to make present and visible.[30] In fact, women’s breasts must inhabit this contradictory space of hiding and revealing at all times. To be read as healthy and normatively-bodied, our culture asks women to reveal that they have breasts via clothing choices and bodily presentation, even as they are expected to cover them. It is acceptable to notice breasts, but not to touch them or refer explicitly to them in public spaces. Women’s breasts represent the dichotomy of forbidden/private and accessible/public that figures many of women’s daily experiences in terms of how their bodies are read and treated by others.
Engelberg captures the ways in which such contradictory expectations of what should be private and public in relation to women’s bodies are reproduced in relation to women’s illnesses such as breast cancer, which is often considered something that is expected to be hidden but also licenses people to cross personal boundaries, drawing attention to that which is usually treated as the unseen seen. In the final panel of this first strip, in which Engelberg draws herself with a shirt that says “Cancer Inside” accompanied by an arrow pointing to her right breast, she draws explicit attention to the surface/depth and hiding/revealing paradoxes that women must negotiate in their self-presentation. Thus it performs disgender by representing Miriam as dissociated or de-centered from her gender identity not because she has cancer, but because of the ways public presentations of cancer create frictions with our normative modes of reinforcing gender embodiment norms, thereby revealing socially disabling aspects of womanhood (i.e. “personal” belongings are also available for public consumption). It also suggests, like Lorde’s memoir, that women’s breast cancer is treated as an aesthetic, superficial or topical problem, rather than a matter of overall mental and physical health, or a matter of life and death. Finally, the shirt is ironic because it does what a great deal of women’s fashion does already—i.e., draw attention to breasts via covering them. In fact, the shirt might as well say “Breasts Inside.” But the disjuncture between “breasts” and “cancer” also does the critical disgendering work of drawing attention to the illness itself, thereby disrupting habitual ways of looking at women’s bodies and the normate expectations for them by making disability and its intersections with gendered expectations more legible.
I would suggest that to some extent racial whiteness that is at work around such normative expectations for hiding/revealing the female body. White women have access to the albeit constricting double expectation of hiding/revealing, whereas women of color’s bodies, particularly but not exclusively African American women’s bodies, have often been either commodified, hypersexualized, and made unsafe, or stripped of legible femaleness as it circulated in dominant culture. This comic can also be read as alluding to Engelberg’s family’s history as Holocaust survivors, though it is not explicit and a reader would need to have read the rest of the comics to make that connection. The words “cancer inside” with the arrow, though marked on the right side of her chest, I would suggest evoke the Stars of David and other triangle-based camp badges that Jewish and other people marked by the Nazi regime were forced to wear on their left breasts. The arrow includes an upside-down triangle, also used in Nazi camps to denote among other things, asocial or gender deviant (later reclaimed by lesbian feminists), mentally ill, and sexually deviant (later reclaimed by the gay rights movement). Thus the image reveals both the privilege of access to racial whiteness as well as the ways this access is complicated and in certain ways denied by Engelberg’s inheritance of racial, gender, and disability trauma through her Jewish heritage.
Engelberg suggests in several comics that she was already living with a certain amount of depression and anxiety before being diagnosed with cancer, which she implicitly connects to her Jewish identity and inheritance of the trauma of genocide. Gabriele Schwab argues that “[t]he damages of violent histories can hibernate in the unconscious, only to be transmitted to the next generation like an undetected disease."[31] Schwab’s language is telling here, as she associates unprocessed trans-generational trauma with an illness not yet diagnosed. In both Engelberg’s and Lorde’s texts, cancer diagnosis and treatment calls to the fore a processing of other inherited traumas. Engelberg’s representation of Jewish identity in part an inheritance of somatic trauma echoes Lorde’s reading of the medicalized experiences of the black female body under white-dominated social and economic systems, as an inheritance of vulnerability. For Lorde, this vulnerability is a positional trauma related to a loss of subjectivity—becoming an object on a table. For Engelberg, relates to inherited fears and anxieties in everyday life that trigger fears of death or illness. For example, Miriam tells us that her parents are “the two most health-conscious people in the entire western world,” constantly mailing her articles about illnesses linked to poor diet, lack of exercise, stress, etc. Thus both authors connect inherited racial trauma to a sense of loss of control over the body. This giving over of control is in part an actual loss—being under anesthesia or not being able to physically do things because of pain or fatigue. It is also a loss of the perception of control—historically as subjects whose health or illness is determined by larger social forces, and in the contemporary moment by becoming aware of the ways their gendered bodies are read by and expected to perform in certain ways for others.
Engelberg’s comics make us aware of the way the normate gaze genders women and reads female-identified bodies as healthy or ill by the approximation to normative aesthetics in their gender performativity. Miriam, after her first round of chemo, is watching a detective show about a doctor who helps sick patients kill themselves. She imagines the detective coming into her house and seeing her lying there bald, watching bad TV and assuming she would be better off dead. “No wait a minute,” she imagines saying, “For all you know I’m just a bald woman watching TV!” Part of the joke here is that there is no broad cultural signification of bald women watching TV except illness—particularly for a white, middle class, professional women. Her bald head already disgenders her body, the illness and assumption that her life is worthless is both an assumption about the worthlessness of the futures of people with disabilities and about a racialized gender non-conforming aesthetic having no other cultural meaning than disability, which then also equates to a future without value. The joke that she could just be a bald woman watching TV is also juxtaposed against earlier references to her parents fleeing Nazi Germany, in which context the idea of a bald woman that a person in authority wants to help kill themselves takes on another set of meanings involving racially, sexually, gender, and disability coded eugenic ideas about whose lives are worth continuing and reproducing. The history of racialized disgendering that Miriam has inherited appears throughout her comics in these uncanny moments of dark humor.
Laura S. Brown argues for a feminist analysis of trauma, which “rather than desensitizing survivors to symptom triggers,” would help people to “reconstruct their world views” such that they can integrate “their painful new knowledge."[32] Engelberg uses humor and suggestion to move toward such a feminist reintegration in the face of additional trauma, though Miriam as a character remains highly ambivalent about her relation to both her gender identity and its history of woundedness as well as that of her Jewish identity as a history of violence. Engelberg’s larger project is attentive to the numerous social-identity-based traumas and disabilities that inform Miriam’s experience, and what those experiences allow her to critique in the present as well as what they open up or foreclose in terms of conceptions of the future. Cathy Caruth argues that trauma is not only historically but also future oriented, in that what remains unassimilable in the past directly affects the ways we imagine possible futures (Listening xiv).. Engelberg’s comic series as a whole links aspects of ethnic, gender, and disability identity that have been unconscious or unassimilable to the possibility for other kinds of futures—futures that are less certain but in which Miriam can become more aware of (and possibly more able to integrate) many of the disabling narratives of her broader culture—including the repression of the knowledge of women’s oppression and the devastating effects on Jewish people of the history of anti-Semitism, including the Holocaust.
Miriam’s ambivalent relation to and at times seemingly unconscious articulation of historical and contemporary trauma is a way of negotiating a recognition of historical woundedness without inhabiting a victimized identity or equating disability or impairment with an irredeemably negative state of being. One “danger of emphasizing memory and mourning lies in using trauma as the foundation of identity,” Schwab writes. “Such attachment to injury is problematic, especially in a ‘wound culture’ oversaturated with stories and studies of trauma. An excessive emphasis on mourning may indeed contribute to an identitarian definition of cultural belonging by tying identity to victimization.”[33] This logic of an oversaturation of trauma, however, can reinforce dominant narratives that suggest that women’s everyday experiences of fear and oppression are not traumatic because they are a normalized part of our culture. We may not be oversaturated with stories of trauma, but with trauma itself. As Laura Brown points out, many of the traumatic experiences of women in our society are not uncommon; in fact the threat of trauma is a daily, or what is now commonly referred to as insidious trauma. Insidious trauma “shapes a worldview rather than shatters assumptions about the world,” but nevertheless may result in “symptomology similar to that of direct or indirect trauma” (Root 240).[34] Using Brown’s lens of normative cultural traumas and Engelberg’s references to a more commonly acknowledged social and cultural trauma—the Holocaust—we can begin to read Engelberg’s presentation of gender itself as disabling not only in terms of access to income, authority, and freedoms, but also in terms of mental health. Racialized disgendering is itself an ongoing set of culturally acceptable microaggressions as well as a “lifetime risk of exposure to certain trauma."[35] Miriam’s desire not to present an “excessive emphasis” on mourning or victimization leads to ambivalence over her own minority social positions and self-critiquing of her own thoughts and feelings around her illness. It is only in relation to her inhabiting of a potentially physically and emotionally traumatizing position—that of the body diagnosed with what is likely a terminal illness—that the text becomes more able to articulate the traumatic aspects underlying gender itself, thereby making the reader more aware of gender as racialized disgender.
Looking on the Dark Side of Things: Disgender and Disabled Futures
Lorde and Engelberg both represent racialized disgender as a rethinking of the ideological role of the logic of futurity for bodies identified as wounded or vulnerable. The body that registers publically as racially disgendered, and thus potentially makes the broadly shared state of racialized disgender more perceptible to others, resists normative future-oriented medical narratives in that racialized disgender exists in relation to the body as a both a disruptive condition and simultaneously a condition that is not available for elimination, rehabilitation, or cure. As long as race and gender are constructed via idealized bodily norms and the reproduction of heteronormativity, racism, patriarchy, and other systems of power and privilege, there will be racialized disgender. Those structures can change, but the individual body itself can be neither the agent nor the site of that change. In the case of diagnoses of breast cancer, the medical prognosis often “operates to actively position the subject in relation to the precarious roulette of futurity” as a body “having diverged from normal operation” which needs to be put back on a proper future-oriented track.[36] The path to futurity becomes one of individual recovery rather than a recognition of not only the systemic causes of cancer but also the continued disabling of bodies marked female and sick within current future-oriented, ableist, developmental, curative, progressive models of both gender equity and medical recovery.
As several critics of dominant rhetorics of breast cancer have noted, discourses surrounding breast cancer awareness campaigns function to individualize and naturalize breast cancer, as well as to create a safe space for corporations to present themselves as “doing something for women, without being feminist.”[37] Multiple and intersecting gendered discourses surrounding breast cancer, its treatment, and its use in corporate culture work to individualize the experience of the disease and to obscure the racial, economic, and gender inequities that make certain bodies more vulnerable to the environmental pollutants that cause the cancer in the first place. This cure-oriented and palatable pinkwashing also leaves no room for those whose cancer has metastasized and who no longer fit the medical model of progression toward a normative or “healthy” future. Emily Waples notes of Engelberg’s memoir, “its end point of metastasis, rather than a return to health and ‘normalcy,’ highlights the disease’s complicated, and terrifying, relationship to temporality."[38] Contra the individualizing white-dominated discourses of corporate breast cancer and positive narratives of recovery, both Lorde’s and Engelberg’s texts suggest that broader social structures of systemic inequality and narrative structures of normalizing futurity must change, not the individual ill body.
Normative, racialized sex-gender systems often function conservatively as a site for the ideological reproduction of power. This has been true throughout U.S. history, certainly, in the case of ideals of true womanhood, white legal rights to the offspring of black slaves, the American eugenics movement, the legal sterilization of women of color and people with disabilities, anti-miscegenation laws, as well as the restriction of legal access to marriage and parental rights (not to mention bathrooms) for black, gay, lesbian, queer, and transgender people. Such discourses about who has access to legally legitimate and institutionally supported gender and sexual identities are often framed in relation to an idealized but never realized future. Lee Edelman argues that our current understanding of the political holds out a heteronormative fantasy of the future that figures the white, female, middle-class child as a symbol of our cultural vulnerability and possibility, in need of protection to ensure the stability of our future. This version of the political future reinforces conservative and anti-queer modalities of being as the only ways of being that enable positive and valuable futures.
Racialized disgender as a way of reading social identity can help us rethink the connection between marginalized social positions and logics of futurity such as Edelman’s description of conservative heteronormative reproductive futurity. In Lorde’s and Engelberg’s narratives attentiveness to racialized disgender helps the reader to reimagine a connection between wounded pasts and futures that might be disabled but are nonetheless worth living and therefore worth investing political energy in. This perspective is figured by both Lorde and Engelberg as one that situates us in relation to the future without it inherently presenting us with a promise, and thus can disrupt the logic of reproductive futurity that devalues and denies futurity to those who do not fit its hegemonic promise—those who are queer, disabled, black, poor, or sick.
This non-promissory future-oriented logic values what we might call looking on the dark side of things. When Lorde does not wear the suggested prosthetic, the representative from Reach for Recovery criticizes her for not “looking on the bright side of things."[39] Lorde experiences this as a disruption of her access to authentic positive thinking and self-validation by demanding a kind of affectation of positive thinking that serves others. “Looking on the bright side of things,” writes Lorde, “is a euphemism used for obscuring certain realities of life, the open consideration of which might prove threatening or dangerous to the status quo.”[40] Lorde’s way of surviving with the knowledge of her wounded experience is to “integrat[e] this crisis into [her] life,” to find ways “to integrate death into living, neither ignoring it nor giving in to it.”[41] As Sarah Ahmed puts it, “looking on the bright side,” can be a way “to avoid what might threaten the world as it is.”[42] Looking on the dark side of things instead might be a way to hold onto aspects of one’s experience that are legitimately painful and traumatic, to make both those experiences and an awareness of their causes a part of oneself and way of living. Such a way of looking might then open a space for an integrated way of experiencing one’s dominant and oppressed positions, and healthy and ill aspects of the self as opposed to a binary perspective that sees one path as healthy and future-oriented in opposition to another path that would involve illness, disability, or oppression and obstructs access to a worthwhile future.
Engelberg is similarly critical of positive narratives of healing or overcoming. She points out the ways in which these narratives set up expectations for women with cancer to perform in exceptional ways such that other people will not have to think about the dark side of things that these women’s bodies represent. Engelberg specifically critiques the ideological work of the word “survivor” as a way of putting a positive affective spin on cancer. “What does [being a survivor] mean, exactly? Is it just a statement of fact?” Miriam asks in the caption to a panel showing a woman wearing a pink ribbon and pointing to a bed out of frame saying “I’m alive, She’s not. Na na nana na!” In the following panel she asks: “or is it a moral judgment?” Here the same woman with the pink ribbon says: “I’m alive because I’m a SURVIVOR. I’ve obviously done all the right things."[43] To be a survivor is to present yourself in contrast and opposition to the sick and the dead, to participate in the narrative that if you have recovered or if you are healthy, if you have no “family history,” if you are a woman who has both breasts and has not yet been raped, assaulted, or otherwise directly traumatized, that you are safe and do not need to think about your own personal or social vulnerabilities and lack of control.[44] And of course Engelberg’s family are survivors of another sort and in the case of being Jewish cannot and would not want to ideologically separate themselves from those who did not survive. Engelberg highlights the ways in which the discourses we impose onto traumas, wounds, and experiences that cause negative affective and bodily responses, attempt to recenter and reassure the not yet ill and (mostly) gender-normative body. Her Jewish identity as descendants of survivors also makes clear that this reassurance is only available for those who begin from the position of not already considering part of their identity decentered and haunted by historical trauma.
Cancer does not mark a change, a better life, or a revelation for Miriam, despite the desires of those around her to turn it into something positive. Cancer is, Engelberg’s memoir suggests, a permanent interruption, similar really to many of the most disabling aspects of our lives and identities. We will not overcome most of the many obstacles, inequities, dependencies, and oppressions we face in our lives. A sense of futurity that only has room for positive narratives of overcoming leaves many people futureless. My focus on the concept of racialized disgender here is an attempt to give more extensive and extended attention to what we think of and experience as the negative aspects of illness, impairment, and socially disabled identities, without assuming that these aspects decrease future possibility or trap us in victimized positions. My hope is that such a focus can show us the ways in which the wounds of our identities have far from exhausted the possible knowledges that they have to offer us.
Works Cited
- Ahmed, Sara. The Promise of Happiness. Durham, NC: Duke UP, 2010.
- Beauboeuf-Lafontant, Tamara. Behind the Mask of the Strong Black Woman: Voice and theEmbodiment of a Costly Performance. Philadelphia: Temple UP, 2009.
- Bordo, Susan. Unbearable Weight: Feminism, Western Culture, and the Body. Berkley: U of California P, 1993.
- Bulter, Judith. “Undiagnosing Gender.” Undoing Gender. New York: Routledge, 2004. 75-101.
- Carby, Hazel V. Reconstructing Womanhood: The Emergence of the Afro-American WomanNovelist. New York: Oxford UP, 1987.
- Caruth, Cathy. Listening to Trauma: Conversations with Leaders in the Theory and Treatment ofCatastrophic Experience. Baltimore: Johns Hopkins UP, 2014.
- Collins, Patricia Hill. “The Sexual Politics of Black Womanhood.” Black Feminist Thought:Knowledge, Consciousness, and the Politics of Empowerment. New York: Routledge, 1999. 123-48.
- Crenshaw, Kimberle. “Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color.” Stanford Law Review. 43.6 (1991). 1241-1299.
- Davis, Lennard. Bending Over Backwards: Disability, Dismodernism & Other DifficultPositions. New York: NYU Press, 2002.
- DeShazer, Mary K. Mammographies: The Cultural Discourses of Breast Cancer Narratives.
- Ann Arbor, MI: University of Michigan Press, 2013.
- --- and Anita Helle. “Theorizing Breast Cancer: Narrative, Politics, Memory.”
- Tulsa Studies in Women’s Literature. 32.2/33.1 (Fall 2013/Spring 2014): 7-23.
- Downs, Jim. Sick From Freedom: African-American Illness and Suffering During the Civil Warand Reconstruction. New York: Oxford UP, 2012.
- Edelman, Lee. “The Future is Kid’s Stuff: Queer Theory, Disidentification, and the Death Drive,” Narrative 6.1 (1998): 18-20.
- Ehrenreich, Barbara. Bright Sided: How the Relentless Promotion of Positive Thinking hasUndermined America. New York: Metropolitan Books, 2009.
- ---.“Welcome to Cancerland: A Mammogram Leads to a Cult of Pink Kitsch.”
- Harper’s Magazine (November 2001): 43-53.
- Engelberg, Miriam. Cancer Made Me A Shallower Person: A Memoir in Comics. New York: Harper, 2006.
- Erevelles, Nirmala. Disability and Difference in Global Contexts: Enabling a TransformativeBody Politic. New York: Palgrave, 2011.
- Garland-Thomson, Rosemarie. Extraordinary Bodies: Figuring Physical Disability in AmericanCulture and Literature. New York: Columbia UP, 1997.
- Harris, Trudier. Saints, Sinners, Saviors: Strong Black Women in African American Literature. New York: Palgrave, 2001.
- Herndl, Diane Price. “Our Breasts, Our Selves: Identity, Community, and Ethics in Cancer Autobiographies.” Signs: Women’s Journal of Women in Culture and Society 32.1 (2006): 221-45.
- ---. “Reconstructing the Posthuman Feminist Body Twenty Years after Audre Lorde’s Cancer Journals.” Disability Studies: Enabling the Humanities. Eds. Sharon L. Snyder, Benda Jo Bruggermann, and Rosemarie Garland-Thomson. New York: Modern Language Association of America, 2002. 144-55.
- Hermes, Joke. Reading Women’s Magazines: An Analysis of Everyday Media Use. Cambridge, UK: Polity Press, 1995.
- Holmes, Martha Stoddard. “Cancer Comics: Narrating Cancer through Sequential Art.” TulsaStudies in Women’s Literature 32.2/33.1 (Fall 2013/Spring 2014): 147-62.
- Lorde, Audre. The Cancer Journals. San Francisco: Aunt Lute Books, 1980.
- ---. Zami: A New Spelling of My Name. Freedom, CA: Crossing, 1982.
- Muñoz, José Esteban. Disidentifications: Queers of Color and the Performance of Politics. U of Minnesota P, 1999.
- Pickens, Therí A. New Body Politics: Narrating Arab and Black Identity in the ContemporaryUnited States. New York: Routledge, 2014.
- Root, Maria P. P. “Reconstructing the Impact of Trauma on Personality.” Personality andPsychopathology: Feminist Reappraisals. Eds. Laura S. Brown and Mary Ballou. New
- York: Guilford Press. 229-265.
- Schultz, Jane E., “Valid/Invalid: Women’s Cancer Narrative and the Phenomenology of Bodily Alteration.” Tulsa Studies in Women’s Literature 32.2/33.1 (Fall 2013/Spring 2014): 71-87.
- Spillers, Hortense. “Mama’s Baby, Papa’s Maybe: An American Grammar Book.” Diacritics 17.2 (1987): 64-81.
- Waples, Emily. “Avatars, Illness, and Authority: Embodied Experience in Breast Cancer Autopathographics.” Configurations 22.2 (Spring 2014): 153-181.
Endnotes
- Thank you to Jennifer Ashton, Andrea Gadberry, Kristen Proehl, Jean Wyatt and the reviewers from Genders for their insightful feedback on previous versions of this essay.
- Audre Lorde, The Cancer Journals (San Francisco: Aunt Lute Books, 1980), 10.
- Hortense Spillers, “Mama’s Baby, Papa’s Maybe: An American Grammar Book,” Diacritics 17.2 (1987): 64-81. Kimberly Crenshaw, “Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color,” Stanford Law Review 43.6 (1991): 1241-1299. Patricia Hill Collins, “The Sexual Politics of Black Womanhood,” Black Feminist Thought: Knowledge, Consciousness, and the Politics of Empowerment (New York: Routledge, 1999), 123-48.
- Hortense Spillers, “Mama’s Baby, Papa’s Maybe: An American Grammar Book,” Diacritics 17.2 (1987): 77.
- Spillers, 80.
- Rosemarie Garland-Thomson, Extraordinary Bodies: Figuring Physical Disability in American Culture and Literature (New York: Columbia UP, 1997), 103-104.
- Nirmala Erevelles, Disability and Difference in Global Contexts: Enabling a Transformative Body Politic (New York: Palgrave, 2011), 38-39.
- José E.
- Diane P. Herndl, “Our Breasts, Our Selves: Identity, Community, and Ethics in Cancer Autobiographies,” Signs: Women’s Journal of Women in Culture and Society 32.1 (2006): 27 and 28 and Erevelles, 6 and Iris Marion Young, On Female Body Experience: “Throwing like a Girl” and Other Essays (Oxford University Press, 2004) and Spillers and Susan Bordo, Unbearable Weight: Feminism, Western Culture, and the Body(Berkley: U of California P, 1993) and Tamara Beauboeuf-Lafontant, Behind the Mask of the Strong Black Woman: Voice and the Embodiment of a Costly Performance (Philadelphia: Temple UP, 2009). Young argued as early as 1980 that “women in sexist society are physically handicapped” (152) in that they learn from a young age to “actively to hamper [their] movements” and live in constricted space (153). Iris Marion Young argued as early as 1980 that “women in sexist society are physically handicapped” (152) in that they learn from a young age to “actively to hamper [their] movements” and live in constricted space (153). As mentioned above, Hortense Spillers argues that the denial of legalized gender status to Africans forcibly brought to the U.S. was used to limit the personhood of blacks in America through the denial of legalized family rights and the corresponding heteronormative gendered subjectivities that attend those rights. Susan Bordo has demonstrated the ways in which agoraphobia, hysteria, and anorexia have been both created by cultural expectations for white middle-class women as well as being hyperbolic, visible, and disruptive of gender norms. Diane Herndl notes that the emergence of the white “invalid woman” in the mid-19th century constructed ideals of womanhood through standards of modesty that left white women ignorant of their own bodies; restrictive and debilitating clothing styles; and parental and medical practices that deprived girls of protein-rich foods, exercise, and hygiene (27-28). As I discuss in more detail below in relation to Lorde, Tamara Beauboeuf-Lafontant suggests that the cultural myth of the strong black woman results in illness for many actual black women. Erevelles argues that disability is the “ideological lynchpin” used to “(re)constitute social difference along the axes of race, gender, and sexuality in dialectical relationship to the economic/social relations produced within the historical context of transnational capitalism” (6).
- This cooptation is reflected in media and other popular cultural discourses that frame all trans* people as simply born in the wrong body, and “fixable” via hormones and surgery. This binary discourse has been adopted by some trans* people for whom it may not fit but who desire a diagnosis that will give them access to the insurance coverage that would make a physical transition possible.
- Poor women, women of color, immigrant or foreign women, and others who do not fit dominant middle-class white American models of femininity have been dehumanized and disenfranchised via a number of ungendering rhetorics that make these women’s bodies into exchangeable labor sources rather that citizens with liberal personhood. At the same time, the rhetorics that endow one with legible gender are also in themselves frequently socially disabling—whether they evolve out of the model of the weak, dependent white mistress, the asexual caretaking black mammy, or any other number of racist and classist narratives about womanhood.
- Anita Helle, “Theorizing Breast Cancer: Narrative, Politics, Memory,” Tulsa Studies in Women’s Literature 32.2-33.1 (Fall 2013/Spring 2004): 8.
- Lorde, 7.
- Lisa Diedrich, Treatments: Language, Politics, and the Culture of Illness (University of Minnesota Press, 2007), 65.
- Hazel V. Carby, Reconstructing Womanhood: The Emergency of the Afro-American Woman Novelist (New York: Oxford UP, 1987) and Bonnie Thorton Dill “The Dialectics of Black Womanhood” for foundational discussions on the dominant ideologies of black womanhood in the United States as they evolved from the system of chattel slavery in which black woman functioned as property, laborers and the reproducers of property and labor.
- Therí A. Pickens, New Body Politics: Narrating Arab and Black Identity in the Contemporary United States (New York: Routledge, 2014), 142.
- Trudier Harris, Saints, Sinners, Saviors: Strong Black Women in African American Literature (New York: Palgrave, 2001), 11 and 20. Harris argues that the historical stereotype of the strong black women makes its way into contemporary African American literature via positive representations of big, powerful black woman “who [are] more suprahuman than human” (11), but whose strength comes at a cost, “sometimes handicap[ping] the very tradition it seeks to perpetuate” (20).
- Lorde, 33.
- Lorde, 13.
- Lorde, 35.
- Barbara Ehrenreich, “Welcome to Cancerland: A Mammogram Leads to a Cult of Pink Kitsch,” Harper’s Magazine (November 2001): 52.
- Ehrenreich, 46.
- Lorde, 41.
- Lorde, 58.
- Lorde, 58.
- Lorde, 58.
- Jim Downs, Sick From Freedom: African-American Illness and Suffering During the Civil War and Reconstruction (New York: Oxford UP, 2012), 14.
- Downs, 127.
- Lorde, 61.
- Breast cancer awareness campaigns make use of this simultaneous presence/absence of women’s breasts by making shirts and signs that draw attention not only to the existence of breast cancer but the breasts themselves. Shirts that say things like “Support My Rack” and “Yes, They’re Fake. The Real Ones Tried to Kill Me,” play on the simultaneous visibility and covering of women’s breasts as well as the interstitial space breasts occupy between public and private embodiment.
- Gabriele Schwab, Haunting Legacies: Violent Histories and Transgenerational Trauma (Columbia University Press, 2010), 14.
- Laura S. Brown, “Not Outside the Range: One Feminist Perspective on Psychic Trauma,” Trauma: Explorations in Memory, ed. Cathy Caruth (Baltimore: John Hopkins UP, 1995): 109 and 110.
- Schwab, 19.
- Maria P. P. Root, “Reconstructing the Impact of Trauma on Personality,” Personality and Psychopathology: Feminist Reappraisals, eds, Laura S. Brown and Mary Ballau (New York: Guilford Press), 240. Interestingly, Root includes generational trauma (such as descendants of Holocaust survivors), minority social positioning (including heterosexism), and the experience of declining health or progressive illness under insidious trauma—all three central disabilities addressed in Engelberg’s work and all three of which intersect significantly with the others (241).
- Brown, 108.
- Nadine Ehlers, “The Dialectics of Vulnerability: Breast Cancer and the Body in Prognosis,” Configurations 22.1 (Winter 2014): 123.
- Ehrenreich, 48. Ehrenreich has noted that the “cult of pink Kitsch” hyper-feminizes and infantilizes breast cancer patients, while ignoring its causes. Jain presents a similar critique of “pinkwashing,” i.e. “the use of pink [in relation to] breast cancer by industries to build good will, move product, and cover up their production of carcinogens” (519).DeShazer and Halle note the emergence of critiques of breast cancer rhetoric since 2000 that “challenge mainstream cancer culture for its corporate complicity, pink iconography, upbeat rhetoric, and privileging of philanthropy over activism” (8).
- Emily Waples, “Avatars, Illness, and Authority: Embodied Experience in Breast Cancer Autopathographies,” Configurations 22.2 (Spring 2014), 158-159.
- Lorde, 57.
- Lorde, 76.
- Lorde, 8.
- Sara Ahmed, The Promise of Happiness (Durham, NC: Duke, 2010), 83.
- Engelberg, “Survivor”
- Ehrenrich, 50. Ehrenrich goes so far as to call the cult of survivorhood a “mass delusion” that “down-play[s] mortality and promot[es] obedience to medical protocols known to have limited efficacy.”